ACADEMIC EMERGENCY MEDICINE • November 2000, Volume 7, Number 11
1271
were noted. No further attempt was made prior to ment are not infallible, and providers should be
transport to confirm tube placement or address the aware of multiple methods to confirm proper place-
difficulty in ventilating the patient. The inability ment. It is recommended that trauma systems de-
to detect breath sounds in a moving helicopter or velop appropriate protocols for the out-of-hospital
ambulance has been noted; therefore, it is imper- and ED settings, and continuously review these
ative that the emergency care provider be certain protocols to safeguard our patients.
as to the proper positioning of the ETT prior to
2
0,21
transport.
It appears that the flight crew was References
relying on color capnometry to confirm the tube
placement and wished to facilitate transport to the
trauma center. Although there was a relatively
1
. Roberts JR, Hedges JR. Clinical Procedures in Emergency
Medicine. 3rd edition. Philadelphia: W. B. Saunders, 1998, pp
9–44.
3
short flight time, 13 minutes may represent a sig- 2. Van Stralen DW, Roger M, Perkin RM, Fea S. Retrograde
intubation training using a mannequin. Am J Emerg Med.
nificant delay in not providing adequate ventila-
1
3
995; 13:50–2.
tion to a patient with an acute head injury.
. King HK. Airway management of patients with maxillofa-
During the flight, difficulty in bagging the pa- cial trauma. Acta Anesthesiol Sin. 1996; 34:213–20.
4
. Parmet JL, Colonna-Romano P, Horrow JC, Miller F, Gon-
tient became more pronounced. The concern at this
time was for the possibility of a tension pnemo-
thorax, and despite good oxygen saturation and he- cheal intubation along with difficult mask ventilation. Anesth
modynamically stable vital signs, bilateral needle
decompressions were performed. It does not ap-
pear that other causes of difficult bagging (malpo- 6. McNamara RM. Retrograde intubation of the trachea. Ann
zales J, Rosenberg H. The laryngeal mask airway reliably pro-
vides rescue ventilation in cases of unanticipated difficult tra-
Analg. 1998; 87:661–5.
5
. Barriot P, Riou B. Retrograde technique for tracheal intu-
bation in trauma patients. Crit Care Med. 1998; 16:712–3.
Emerg Med. 1987; 16:680–2.
sitioned tube, plugging with secretions) were con-
7. Audenaert SM, Montgomery CL, Stone B, Akins RE, Lock
sidered. Perhaps if suctioning had been attempted
RL. Retrograde-assisted fiberoptic tracheal intubation in chil-
the malposition of the tube would have been iden- dren with difficult airways. Anesth Analg. 1991; 73:660–4.
. Cooper CM, Murray-Wilson A. Retrograde intubation. Man-
agement of a 4.8kg, 5-month infant. Anesthesia. 1987; 42:
8
tified.
Upon arrival to the ED, bilateral chest tubes 1197–200.
9
. Stern Y, Spitz T. Retrograde intubation of the trachea. J
Laryngol Otol. 1991; 105:746–7.
0. Shantha TR. Retrograde intubation using the subcricoid
were placed. This is appropriate in the setting of
significant trauma where needle decompressions
were already performed. When the chest x-ray region. Br J Anesth. 1992; 68:109–12.
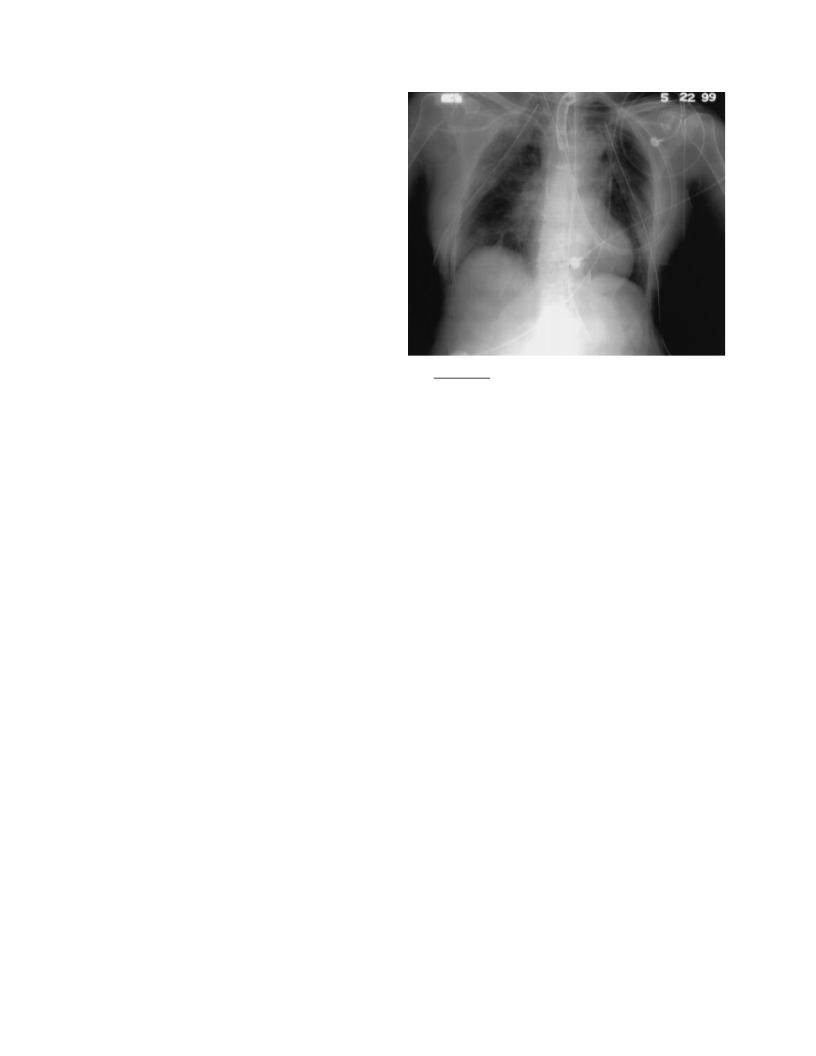
1
1
1. Dhara SS. Retrograde intubation—a facilitated approach.
failed to identify a properly positioned ETT (Fig.
), an anesthesia consult was obtained. This cre-
Br J Anesth. 1992; 69:631–3.
1
12. Bowes WA, Johnson JO. Pneumomediastinum after
ated a further delay in managing the airway. It is planned retrograde fiberoptic intubation. Anesth Analg. 1994;
7
8:795–7.
unclear why the nonfunctioning tube was not im-
mediately removed and attempts to secure a pat-
ent airway were not made.
1
3. Hung OR, al-Qatari M. Light-guided retrograde intuba-
tion. Can J Anesth. 1997; 44:877–82.
14. Lechman MJ, Donahoo JS, Macvaugh H. Endotracheal in-
tubation using percutaneous retrograde guidewire insertion
followed by antegrade fiberoptic bronchoscopy. Crit Care Med.
Two of the most important predictors of mor-
tality in trauma patients are the GCS and the re-
1
986; 6:589–90.
2
2
spiratory rate. It is imperative to determine that 15. Arndt GA, Topp J, Hannah J, McDowell TS, Lesko A. In-
tubation via the LMA using a Cook retrograde intubation kit.
the severely head-injured patient is maintaining
good oxygenation and ventilation to minimize sec-
ondary injury to the brain. The physician and EMS larynx produced by resuscitative intubation. Am J Forens Med
personnel should be aware of alternative methods
of establishing a definitive airway, such as RI, in
the patient with the difficult airway. A recent study outcomes. Am J Emerg Med. 1996; 14:617–9.
Can J Anesth. 1998; 45:257–60.
16. Raven KP, Reay DT, Harruff RC. Artifactual injuries of the
Pathol. 1999; 20(1):31–6
1
7. Karch SB, Lewis T, Young S, Hales D, Ho CH. Field in-
tubation of trauma patients: complications, indications, and
1
8. Falk JL, Sayre MR. Confirmation of airway placement.
has shown that the experiences and availability of
devices for difficult airway management varies
Prehosp Emerg Care. 1999; 3:273–8.
19. Salem MR, Wafai Y, Joseph NJ, Baraka A, Czinn EA. Ef-
across EM residency programs and among pro- ficacy of the self-inflating bulb in detecting esophageal intu-
bation. Does the presence of a nasogastric tube or cuff deflation
gram directors, with RI kits found only in 35% of
make a difference? Anesthesiology. 1994; 80(1):42–8.
2
3
the programs reviewed.
20. Brown LH, Gough JE, Bryan-Berg DM, Hunt RC. Assess-
ment of breath sounds during ambulance transport. Ann Emer
Med. 1997; 29:228–31.
CONCLUSIONS
2
1. Hunt RC, Bryan DM, Brinkley VS, Whitley TW, Benson
NH. Inability to assess breath sounds during air medical trans-
port by helicopter. JAMA. 1991; 265:1982–4.
This case demonstrates a possible complication of
using RI. Additionally, it illustrates the need for
emergency professionals to be aware of potential of a national survey. Ann Emerg Med. 1999; 33:694–8.
complications and methods to ensure that the pro-
cedures they perform are done correctly. As seen
above, adjuncts available to confirm ETT place- 76–81.
2
2. Levitan RM, Kush S, Hollander JE. Devices for difficult
airway management in academic emergency medicine: results
2
3. Hannan EL, Farrell LS, Bessey PQ, Cayten CG, Cooper A,
Mottley L. Accounting for intubation status in predicting mor-
tality for victims of motor vehicle crashes. J Trauma. 2000; 48:

 Fichter
Fichter