The Laryngoscope
Lippincott Williams & Wilkins, Inc., Philadelphia
©
2002 The American Laryngological,
Rhinological and Otological Society, Inc.
Immediate Reconstruction of Extruded
Alloplastic Nasal Implants With Irradiated
Homograft Costal Cartilage
J. Madison Clark, MD; Ted A. Cook, MD
Objective: To describe a novel surgical protocol
for the management of patients presenting with ex-
truded nasal implants. Study Design: Retrospective
chart review. Methods: Analysis of consecutive pa-
tients presenting with extruded nasal implants from
this series of patients, a novel surgical protocol was
used. The extruded implant was removed and imme-
diate reconstruction with irradiated rib cartilage was
done. All patients were evaluated for postoperative
infection, graft extrusion, and satisfaction with cos-
metic result. There was one major complication in
this series of 18 patients, warping of the IHCC, which
necessitated removal and replacement. This approach
appears to be a reasonable method for reconstruction of
extruded nasal alloplasts. Key Words: Implants, ex-
troded, nasal reconstruct.
1986 to 2000. Patients were selected from a large da-
tabase of revision rhinoplasty cases. Inclusion crite-
ria were: 1) at least one previous rhinoplasty proce-
dure, 2) an extruded nasal implant that was
documented preoperatively, 3) immediate recon-
struction that was carried out with irradiated ho-
mograft costal cartilage (IHCC), and 4) at least 1 year
of follow-up recorded, including standard postopera-
tive rhinoplasty photographs. A total of 18 patients
met the inclusion criteria and form the basis of this
study. Data gathered from the charts included date of
surgery, last date of follow-up, location of implant
extrusion, alloplastic material, specific use of IHCC
for reconstruction, percent of clinical IHCC resorp-
tion at last follow-up, and presence of warping of the
IHCC. Results: All 18 patients were satisfied with the
cosmetic outcomes of their nasal reconstructions. The
most common extruded alloplast was Silastic, fol-
lowed by Gore-Tex (W.L. Gore & Associates, Inc., Flag-
staff, AZ). There were no cases of extrusion or infec-
tion of the IHCC implant subsequent to immediate
reconstruction of the extruded alloplast. Clinical re-
sorption of the IHCC was minimal, with a mean
follow-up of 26 months. Only one patient had a com-
plication, warpage, resulting in removal of the IHCC.
In that patient, the IHCC still had carving markings
on the implant after 2 years in vivo. Conclusions: In
Laryngoscope, 112:968–974, 2002
INTRODUCTION
Alloplastic materials have been used in nasal dorsal
augmentation and structural reconstruction for many
years. Most alloplastic materials have been abandoned in
the United States and Europe because of the high rates of
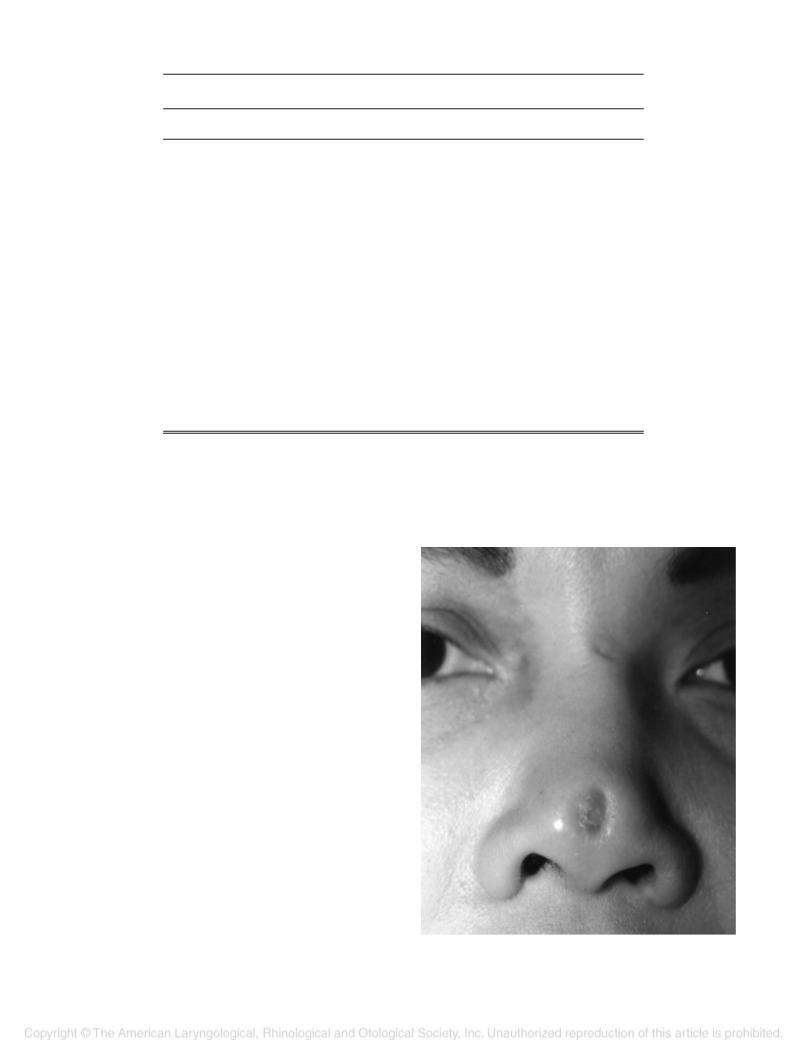
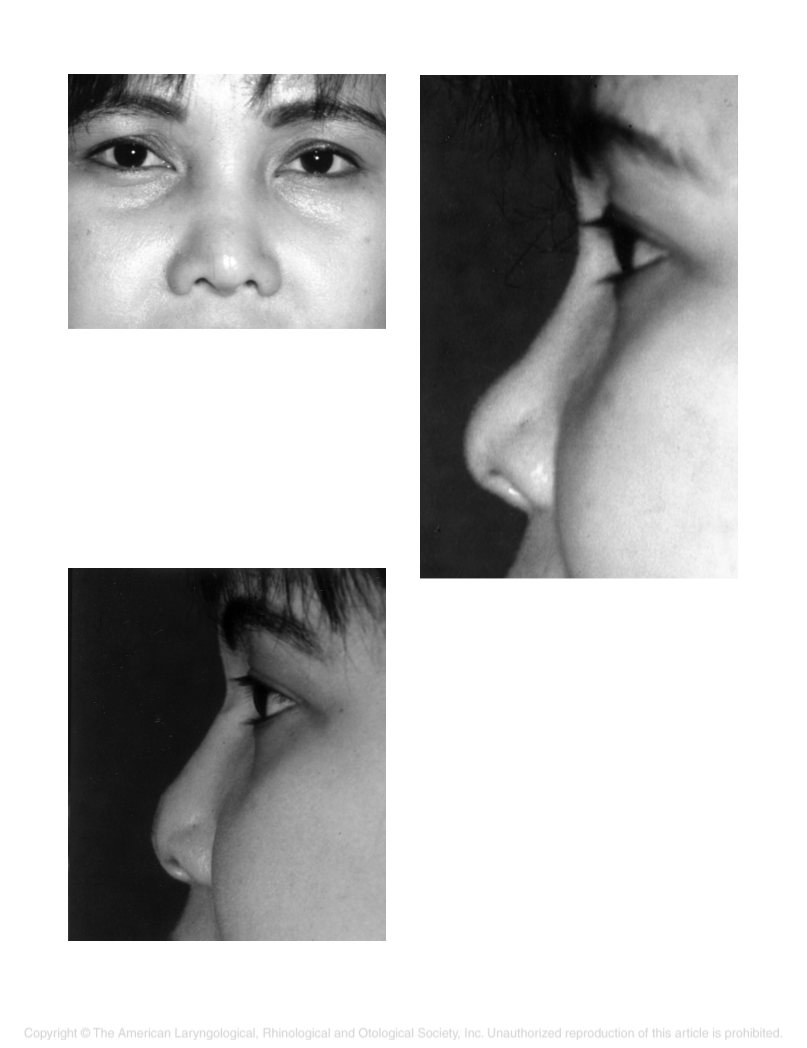
infection or extrusion. Alloplastic implants for dorsal pro-
jection and narrowing, primarily made of medium-density
Silastic do, however, remain popular throughout Asia,
particularly in Thailand and Japan. Thus, patients who
have previously had implants inserted in these countries
continue to be seen in this country (Figs. 1–7). The most
devastating complication, extrusion, has been well de-
scribed in the literature, with rates of extrusion varying
with the experience of the surgeon, length of follow-up,
1–3
and the composition of the alloplast.
The treatment of extruded nasal implants is complex.
Removal of the alloplastic implant, the nidus of infection,
is paramount. Antibiotics are generally recommended,
certainly if infection is clinically present. The dilemma in
the authors’ minds has been what to do with the defect left
by removal of the implant and the appropriate timing of
reconstruction.
Presented at the Annual Meeting of the Triological Society, Palm
Desert, CA, May 15, 2001.
From the Division of Facial Plastic and Reconstructive Surgery,
Department of Otolaryngology/Head and Neck Surgery (J.M.C.), The Med-
ical University of South Carolina, Charleston, South Carolina; and the
Division of Facial Plastic and Reconstructive Surgery, Department of Oto-
laryngology/Head and Neck Surgery (T.A.C.), Oregon Health Sciences Uni-
versity, Portland, Oregon, U.S.A.
Traditional methods of management of extruded im-
plants usually involve removal of the implant to allow
resolution of inflammation and then reconstruction at a
4
later date. Patients are frequently devastated, not only
Editor’s Note: This Manuscript was accepted for publication March
1, 2002.
about the extrusion, but also about their appearance while
they are “unreconstructed” to allow for resolution of in-
flammation. Moreover, the skin/superficial muscular apo-
neurotic system (SMAS) envelope inevitably contracts
down to the void left by the removal of the implant. In a
1
Send Correspondence to J. Madison Clark, MD, Assistant Professor,
Division of Facial Plastic and Reconstructive Surgery, Department of Oto-
laryngology/Head and Neck Surgery, The Medical University of South
Carolina, 150 Ashley Avenue, Charleston, SC 29401-5803, U.S.A. E-mail:
Laryngoscope 112: June 2002
Clark and Cook: Immediate Reconstruction of Extruded Alloplastic Nasal Implants
9
68

 Watanabe
Watanabe